
My thanks to advocate Eileen Holderman for her consultation on this blog post
The US government health agencies and some organizations who purport to represent people with ME (pwME) are deceiving this community by purposefully conflating names and criteria for myalgic encephalomyelitis (ME), and the government constructs chronic fatigue syndrome (CFS) and systemic exertion intolerance disease (SEID). These organizations are complicit with carrying out the government’s nefarious actions in burying a severe neurological disease, ME, which has killed and rendered hundreds of thousands of Americans severely disabled for many decades.
HHS is Adopting SEID Criteria While Cloaking with ME Name
In defiance of ME stakeholders, the Chronic Fatigue Syndrome Advisory Committee (CFSAC), ME expert doctors and researchers, advocates, and patients, the U.S. Department of Health and Human Services (HHS) has consistently refused to adopt the name myalgic encephalomyelitis with its definition created by ME experts (the latest one being the International Consensus Criteria (ICC)) for the distinct disease. HHS admits that the disease ME, as classified by the World Health Organization (WHO) as a neurological disease since 1969, exists as distinctive and unequal to CFS and SEID, yet they refuse to formally recognize it, adopt its proper name and criteria, fund it and educate about it.
Why would HHS state that ME exists yet deny care for the people suffering from the disease? There is no question that since the 1980’s there has been an HHS agency-wide effort to cover up facts about ME, including the dozens of outbreaks of ME worldwide. Once they have started on the path of erasing history, HHS cannot politically afford to change course. Unless exposed publically or challenged legally, HHS will not admit to their malfeasance of attempting to erase a disease and therefore they keep inventing new vague umbrella entities with demeaning names to cover up their wrongful actions.
Organizations Are Adopting SEID Criteria While Cloaking it with ME Name
Some organizations purport to advocate for pwME yet, deceptively, aid the government with the creation, promotion, and dissemination of faulty definitions (SEID being the latest one) and with the conflation and misusing of names. Ironically, they falsely label themselves as ME organizations when in fact they do not advocate for the disease myalgic encephalomyelitis.
These organizations get preferential treatment from the government for their partnership with them. They get funding for research projects and are rewarded with a seat at the government table. They are selected to serve on government working groups where they are in place to advise the government on policy decisions. The government also partners with film production companies or organizations to show screenings of their film.
Additionally, HHS arranges private meetings with these organizations where they can meet with high-level government officials. For example, Dr. Lily Chu, vice president of the IACFSME organization, consulted privately with Donna Pickett of NCHS/CDC (the National Center for Health Statistics – the agency is overseen by the CDC and is in charge of coding) to work on proposals for changes to US ICD coding.
Their consultation led to a presentation of their proposal in a public meeting on September 12, 2018. This ‘public’ meeting was unannounced to the rest of the “public”. Therefore, Dr. Chu was able to call in her comments and endorsement of a harmful, unscientific proposal without any challenge from the rest of the community. Sneaky much?
Classifying SEID as if Equal to ME
According to Donna Pickett of NCHS/CDC and Dr. Chu, all HHS agencies have currently adopted the untested SEID. At the same time, HHS is using the combination acronym ME/CFS – when in fact SEID is not ME nor is it CFS (this was clarified in the 2015 IOM report)!
The nomenclature deception is purposeful and really serves to confuse and conflate everything into a chaotic mess where names and definitions have lost all meaning. The government’s hope is that by the wrongful use of the ME/CFS acronym, it will lull pwME into thinking that ME is being included – when in fact it is the farthest thing from the truth.
Listen to Dr. Lily Chu state in her call-in comment at the September 12, 2018, C & M meeting that all HHS agencies have currently adopted and are using SEID.
The current attempt by IACFSME/Chu to elevate SEID by classifying it in the US ICD-10-CM under the same heading as ME – as if it is an equal neurological disease – when clearly it is not – is disturbing and dangerous because it will result in the disappearance of ME! (read blog NCHS/CDC Proposal for ICD-10-CM). Other countries should pay attention because whatever happens in the US usually is followed by other countries.
The organization MEadvocacy who has never wavered from their mission to advocate for the disease ME as defined by ME experts has taken action and submitted comments to object to the NCHS/CDC and IACFSME/Chu proposal. You can read about their submitted comments here.
Solve ME/CFS Initiative was repeatedly asked by longtime independent ME advocate and past CFSAC voting member, Eileen Holderman, on Twitter what Solve’s response to the dangerous ICD-10-CM proposal was. It was first met with silence, then with a curt reply. Eventually, Solve sent out this video featuring their CEO, Carol Head.
In this 3 minute video, Carol Head states: “We work with the CDC regarding ICD coding.” Does SMCI work with CDC behind our backs in secrecy? Did SMCI help write the current proposal for SEID to be classified with ME? We don’t know because there is no transparency in Solve’s actions and they have, to this date, not made an official statement nor revealed if they are submitting comments about NCHS’s proposal for changes to the ICD coding.
*Please note – Finally yesterday Solve ME/CFS Initiative released a policy statement where they openly admit to endorsing the IOM report. The deception and conflation continue and their statement changes nothing written in this blog.
Organizations Hidden Dissemination of SEID
MEAction, Solve ME/CFS Initiative, and Massachusetts ME/CFS & FM Association helped draft a US Senate Resolution for “ME/CFS” featuring the IOM report and its recommendations for the name SEID and the IOM criteria (read the blog Beware of Aiding in the Burial of ME!). When confronted with this betrayal, MEAction issued a clarification on June 28, 2018, deflecting blame and attributing it to confusing language (as of this date, the same language still stands).
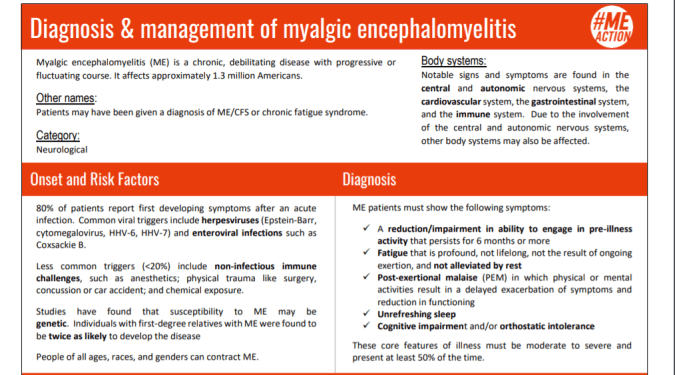
Additionally, MEAction in partnership with #Time for Unrest has created an accredited course for continuing medical education to teach doctors how to diagnose SEID. Their course, deceptively titled Diagnosis & management of myalgic encephalomyelitis, is actually teaching doctors how to diagnose patients using the actual IOM criteria verbatim.
When ME advocates asked Jen Brea on twitter to explain this disparity, her reply was this:

When I further challenged Brea stating that MEAction is currently using IOM/SEID criteria in their educational packets to medical professionals. This was her reply:

So-Called ME Organizations Who Do Not Support ME Experts’ Criteria
I asked MEAction to endorse and promote the #pwME4ICC petition to HHS to recognize and adopt ME as defined by the experts’ criteria – ICC. They countered that they will share it once on social media but could not sign and endorse it because their organization had not come to a decision yet as to which clinical criteria they chose to endorse.
So, MEAction would not sign nor endorse ME-ICC petition, yet they gladly created a curriculum for an accredited continuing education course for medical professionals using IOM/SEID! To endorse the experts’ ME-ICC they need to go through a “community consultation” for which the timeline keeps being delayed but, to endorse and disseminate HHS/IOM’s SEID, they don’t need community approval?
I also approached Solve ME/CFS Initiative asking them to sign and share the petition to HHS for recognition of ME as defined by ICC. They promised to look into it. Three months later Solve has still not replied and have not signed or promoted the ME-ICC petition.
Why This is Important
The topic of which definition is being used for clinical and research purposes as well as correct naming is probably the most critical issue for those representing and advocating for pwME.
The distinct disease myalgic encephalomyelitis as per WHO and experts’ criteria (ICC) is in danger of being totally erased. If you suffer from ME, you will not get a proper diagnosis. Doctors in the US will only know how to diagnose SEID and will give you a SEID ICD code – even though SEID is a definition based on fatigue and 5 subjective common symptoms (with no exclusions for psychiatric conditions).
The definition of ME as per ICC is not a fatigue condition; it is rather a neuro-immune disease with most probably an infectious component. If you are diagnosed with SEID you will not get the proper testing, care, and treatments that would have been geared to a diagnosis of ME.
More disturbingly, IOM/SEID is already being used for research purposes even though the IOM was charged with creating a clinical definition. Some of the new NIH research consortia are using cohorts provided by Dr. Bateman from her clinical practice which have been diagnosed using the IOM/SEID definition.
How to Fight the Disappearing of ME
PwME need to demand change on a federal level. They can do this by joining the 5,178 people who have signed the petition so far to HHS for recognition of ME as defined by our experts’ criteria – the International Consensus Criteria (ICC). They should contact their congressional representatives telling them to press HHS to officially acknowledge their disease ME as defined by ME experts’ criteria – ICC.
PwME should also demand transparency and truthfulness from the organizations that purport to advocate for pwME. PwME should not be left in the dark about what these organizations are planning and supporting. If they are supporting SEID, that means that they are not supporting ME and should openly state so! PwME should demand that any organization that supports SEID should not use the name ME or the conflated name ME/CFS.
#PwME4ICC Are Fighting Back
Hundreds of thousands of Americans suffer from the disabling neuroimmune disease myalgic encephalomyelitis. They have suffered severely for decades. Many have died prematurely. They have lost their health, careers, income, healthcare, family relationships, and friends. On top of that, their own government health agencies refuse to properly and accurately use the experts’ definition and name for their disease. This is malfeasance of the highest order!
Some organizations who should be there for these severely ill patients are the very ones who aid in their betrayal. These organizations are financially supported by the very ill patients they purport to represent – who are often financially destitute. The organizations should be the ones fighting for these patients for recognition of their disease, myalgic encephalomyelitis as defined by ME experts – yet, shamefully – they are doing the opposite.
Activists and people with ME are fighting back against the deception and silencing tactics by HHS and organizations who are complicit with them.
Silence encourages the tormentor, never the tormented. – Elie Wiesel






